Since the first-ever liver transplant was performed in 1963, this operative procedure has been able to improve morbidity and mortality among patients suffering from terminal liver diseases such as hepatocellular carcinoma, hepatitis C virus infection, and alcoholic cirrhosis. Back then, the survival rate, even with liver transplantation, was very low, with none of the first five patients surviving more than 23 days. But in today’s context, the unavailability of adequate donors to match the need is a far greater problem than any technical issue.
There is always a tendency for the body to try to get rid of anything it recognizes to be foreign. This response is mediated via the immune system. This immune response is vital in fending off disease causing organisms such as bacteria, viruses, and sometimes fungi and maintaining the integrity of the various organ systems that make up our body. However, the immune system also sees transplanted organs as foreign objects, which leads to transplant rejection. This article gives you an overview of the action of the Human Immune system and how Tacrolimus, a well established immunosuppressant medication, suppresses it. Also, we hope to address the frequently asked questions by transplant recipients who were just started on Tacrolimus.
Table of Contents
The Immune System
The immune system has two parts, namely the innate immune system and the adaptive immune system. The innate immune system acts non-specifically and rapidly to prevent invaders from entering the body and to eliminate any that already entered. The adaptive immune system has the ability to identify an unlimited repertoire of antigens against which it is able to mount a specific response facilitated by T and B lymphocytes. For this discussion, what is most important is the adaptive immune system.
The Adaptive Immune System
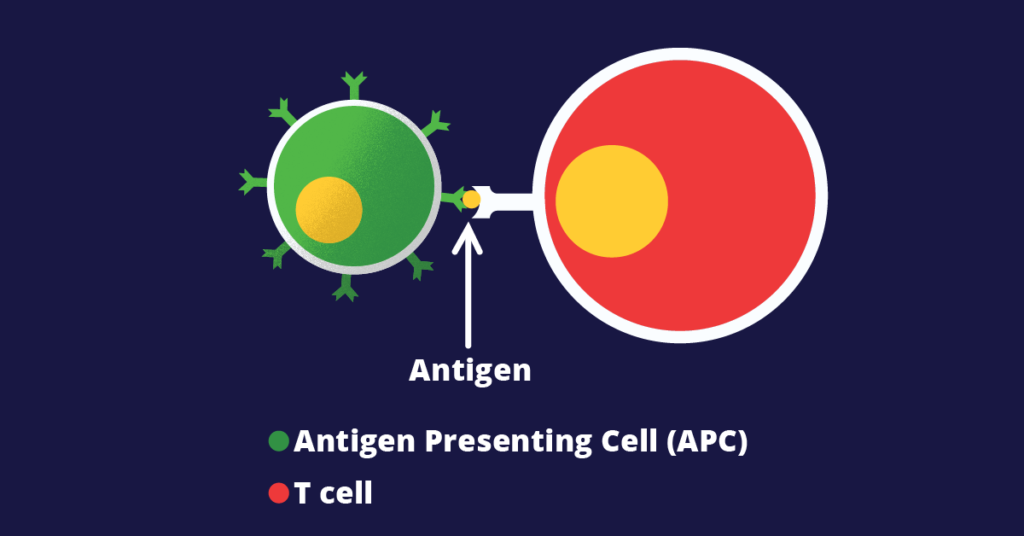
As I mentioned previously, the adaptive immune system can identify a wide range of antigens. There are T cells in lymph nodes with receptors specific to different antigens, which are generated through gene rearrangement during maturation. But T cells cannot identify their respective antigen through direct contact. They are first detected by special kinds of cells called antigen-presenting cells or APCs. These APCs then process the foreign antigens and pass on the information to T cells. APCs have MHC class I and II receptors on their cell surface that they use to present the newly recognized antigens to T cells.
An interaction that takes place between the MHC receptors on APCs and T cell receptors on T cells facilitate the transfer of information. An intracellular pathway, which will be discussed shortly, will subsequently get activated, leading to the release of inflammatory mediators, mainly interleukin-II (IL-II). IL-II is an autocrine activator of T cells. The self-activated T cells will then stimulate the adaptive immune response consisting of cytotoxic T cells, T helper cells, and also antibody-producing plasma cells.
Role of Calcineurin
To understand how Calcineurin and Calcineurin Inhibitors fit in with all of this, it is necessary to peep into the intracellular pathways that connect the signal received from APCs to the release of IL-II. The initial signal received by the T cell receptor will activate a cascade of intracellular events. This begins with the activation of phospholipase C. The action of phospholipase C is to hydrolyze phosphatidylinositol bisphosphate (PIP2) to diacylglycerol (DAG) and inositol triphosphate (IP3), all of which are intracellular messenger molecules.
IP3 increases the intracellular calcium level. Calcium will then bind to calmodulin, forming the calcium-calmodulin complex. The complex will then bind to Calcineurin, which is a calcium-calmodulin complex dependent phosphatase. Now Calcineurin will have gained the ability to dephosphorylate Nuclear Factor of Activated T Cells (NFAT). Dephosphorylation enables NFAT to bind to the IL-II gene inside the nucleus and increase the production of the cytokine. And thus, we can see that Calcineurin plays a vital role in mounting an immune response against any foreign antigen.
Tacrolimus: A Calcineurin Inhibitor
Having talked about the intracellular signal transduction mechanism, now we are at a point where we can understand the action of Tacrolimus. Tacrolimus is a macrolide lactone immunosuppressant isolated from the actinomycete, Streptomyces tsukubaensis. As complex as that may sound, all that is important for us is that Tacrolimus is a Calcineurin inhibitor. To achieve its purpose, first, it binds to the intracellular protein, FKBP12, which then binds to an already formed calcium-calmodulin complex. The entire structure then binds to Calcineurin, thereby inhibiting its phosphatase activity. Steps further down the cascade are also inhibited, resulting in low IL-II production. Thereby T cell activation is reduced, and the activation of the adaptive immune response is limited.
Post-Transplant Period
Transplant recipients receive many medications, sometimes up to 20 pills per day initially. The pill burden may reduce with time, but at least one will have to be continued for life in order to prevent transplant rejection. These new medications following transplant may include immunosuppressants, anti-infectives, and various other medications. Immunosuppressants, as we discussed earlier, help to avoid transplant rejection by the body’s immune system. Anti-infectives are necessary for the early period after organ transplant, where high amounts of immunosuppressants are given, increasing the risk of getting infections substantially.
Tacrolimus Following Liver Transplant
Tacrolimus came into use in the ‘90s as the primary substitute for Cyclosporine to prevent rejection after solid organ transplantation. Tacrolimus has been approved to be used prophylactically as an anti-rejection medication for liver, kidney, heart, and other solid organ transplants in the USA, Europe, and Japan, with an estimate of having been used in over 90% of liver and kidney transplants in 2012. It is also used as a primary rescue immunosuppressant in patients with refractory rejection or intolerance of Cyclosporine.
Other Immunosuppressants
Tacrolimus, however, is not the only known Calcineurin inhibitor. Another drug that has the same action is Cyclosporine. Cyclosporine also inhibits Calcineurin dependent activation of FKBP12 through a different intracellular pathway. Then there are other immunosuppressant medications that suppress the body’s immune system at various phases, such as cell proliferation, receptor interactions, and intracellular signaling. Mycophenolate Mofetil and Azathioprine are some of the other immunosuppressants used to prevent transplant rejection.
Tacrolimus – Properties
Pharmacokinetics
Tacrolimus is a lipophilic drug. Its absorption may be incomplete and highly varied. Its metabolism is mainly mediated by enzymes of the cytochrome P450 system: CYP3A5 and CYP3A4. This could also take a prolonged period of time for some people. Polymorphisms in individuals in cytochrome P450 enzymes can significantly influence prognosis, though it is rarely considered in clinical practice. Its transport is mediated by a P-glycoprotein by an efflux pump mechanism, with predominant excretion via the bile duct.
Dosing and Monitoring
Tacrolimus is usually taken twice a day orally. Unlike over the counter medications, it has to be taken with a gap of exactly 12 hours between doses to ensure a stable level of immunosuppression is achieved at all times. The bioavailability of Tacrolimus is not high and is around 20-25%. It has a variable rate of absorption, which is why it is best taken on an empty stomach minimizing drug-food interactions that can further impair absorption.
With its variable absorption and metabolism, regular monitoring is needed to ensure a constant level of Tacrolimus in the bloodstream. Monitoring should always be done in the morning, and blood should be drawn not more than 1 hour before the morning dose. This allows you to measure the trough level, the lowest level of Tacrolimus that will be present in blood at any time of the day. It is wise to bring a dose of Tacrolimus with you when you come to the laboratory appointment, so you can take the morning dose as soon as the blood is drawn. Like I said, taking the drug on time is very important for a good outcome.
Pharmacogenetics
Pharmacogenetics is the study of genetic factors affecting the variability in drug response due to mutations and polymorphisms. The gene coding for the CYP3A5 enzyme has several alleles. Multiple studies carried out in China, Japan, and Italy have shown that individuals with the CYP3A5*1 genotype have a higher chance of transplant rejection than those with the CYP3A5*3/*3 forms. The dose/concentration ratio was also higher in the latter group. This genotype distribution is largely dependent on ethnicity, which is why Afro-descendants are intermediate or normal metabolizers and have a better pharmacological response and lower need for dosage adjustment than Caucasians.
Adverse Effects
Like any other drug, Tacrolimus comes with its own set of adverse effects. These could present as acute or chronic problems.
Adverse Effects Due to Immunosuppression
Administration of any immunosuppressant presents a chance for infections to set in, sometimes even by less virulent organisms. The infection risk is greatest in the early phases of drug therapy, with most occurring within the first three months after the introduction of the drug. Viral hepatitis, pneumonia, hepatitis, and sepsis are some of the more common complaints. Sepsis is also the most common cause of death in post-transplant patients that occurs due to an effect of the drug. However, the concomitant administration of anti-infective medications reduces the risk of infection and mortality substantially.
An increase in the incidence of neoplasms and post-transplant lymphoproliferative disorders has also been reported, again, especially with the 1st year. More than 21 types of malignancies were observed in a study conducted by the US Multicenter FK506 Liver Study Group, of which the commonest was a lymphoma-like reaction.
Nephrotoxicity
The most common serious adverse effect due to Tacrolimus therapy is acute renal failure. A “kidney function abnormal” designation with abnormalities in the renal function test results is a less severe condition. Both changes were more common in the initial three months of treatment. Acute injury patterns such as acute arteriopathy, thrombotic microangiopathy, and tubular vacuolization, and chronic patterns such as glomerular and interstitial fibrosis, tubular atrophy, focal segmental glomerulosclerosis (FSGS), and arteriolar hyalinization can be seen on histology.
Other Adverse Effects
Tacrolimus has a diabetogenic effect and can also be a cause for newly-onset hypertension. Other side effects include headache, convulsions, gastrointestinal hemorrhages, diarrhea, nausea, and vomiting.
FAQ
What should I do if I miss a dose?
As I mentioned earlier, it is important to take the medication at the correct time in the morning and night, and doses should never be skipped under any circumstance. However, if you were to miss a dose accidentally due to some reason, you should take it as soon as you remember. This does not count, though, if it is almost time for your next dose. Then it should just be omitted. Double dosing is dangerous and should never be done. It is best to call your doctor for advice in a situation you are not sure what to do.
Vomiting right after taking your medication will mean that it has not been absorbed into your system. This is another cause to call your doctor.
How should I store my medications?
It is best to keep your medicines in the original pillboxes as dispensed from the pharmacy. However, it is acceptable to store the pills for the upcoming week in a pillbox if you are on multiple pills. In either case, they should be stored in a cool, dry place out of reach from children and animals.
How will other drugs affect Tacrolimus therapy?
It is best to consult your doctor before taking any over the counter medications, as they could result in various drug interactions. Herbal medicines should be avoided entirely as their drug interactions have not been studied widely and could result in unexpected results.
Does it matter which brand I take?
Protopic and Prograf, among others, are some of the commercial trade names Tacrolimus is sold under. It does not matter which one you go for, but what is important is that you continue to stick to the same one. There are subtle differences between brands, and it is easier to make dose adjustments and maintain a constant blood level if the same product is taken.
References
https://aasldpubs.onlinelibrary.wiley.com/doi/pdf/10.1002/lt.500050611
Calcineurin Inhibitors (Tacrolimus and Cyclosporine) IL2 – Mechanism of action, adverse effects