I have tried my best to simplify the clinical approach to Facial Nerve Palsy. First, I want you to learn the symptoms and signs of facial nerve palsy. We will learn them along with the Facial Nerve Anatomy. Once we identify a Facial nerve palsy, We need to learn how to differentiate upper motor vs lower motor Facial Nerve palsies. Of course, We will have to revise some neuroanatomy again for that. Finally, I will teach you how to localize the site of Facial nerve injury and the responsible causes at each site. I recommend watching my animation about a clinical case of Bell’s palsy to get a basic understanding.
Table of Contents
Symptoms and Signs of Facial Nerve Palsy.

Motor Symptoms
The facial nerve has three types of neuronal components; Motor, Sensory and Parasympathetic. The motor nerve supplies almost all facial muscles from the forehead to the chin. When these muscles are paralyzed, the patients get the following symptoms.
- Inability to blink.
- Drooping of the mouth.
- The disappearance of the nasolabial fold.
- Absence of forehead wrinkles.
Sensory Symptoms.
The sensory Branch supplies the anterior ⅔ of the tongue, which results in altered taste sensations. I will not discuss clinically less-important nerve supplies such as the posterior auricular area.
Autonomic Symptoms.
The facial nerve provides parasympathetic fibers to the lacrimal glands and to some salivary glands. Without tears, eyes are prone to ulcerations and infections.
Upper motor vs Lower motor Facial nerve weakness.
The facial nerve arises from the Pons of the brain stem. So any lesion at or below the level of Facial nerve nuclei produces paralysis of the full side of the face.
Facial nuclei receive signals from the Cerebral cortex. Look at the diagram below for clarification. What would happen if there was a stroke at one part of the brain (cortex)?
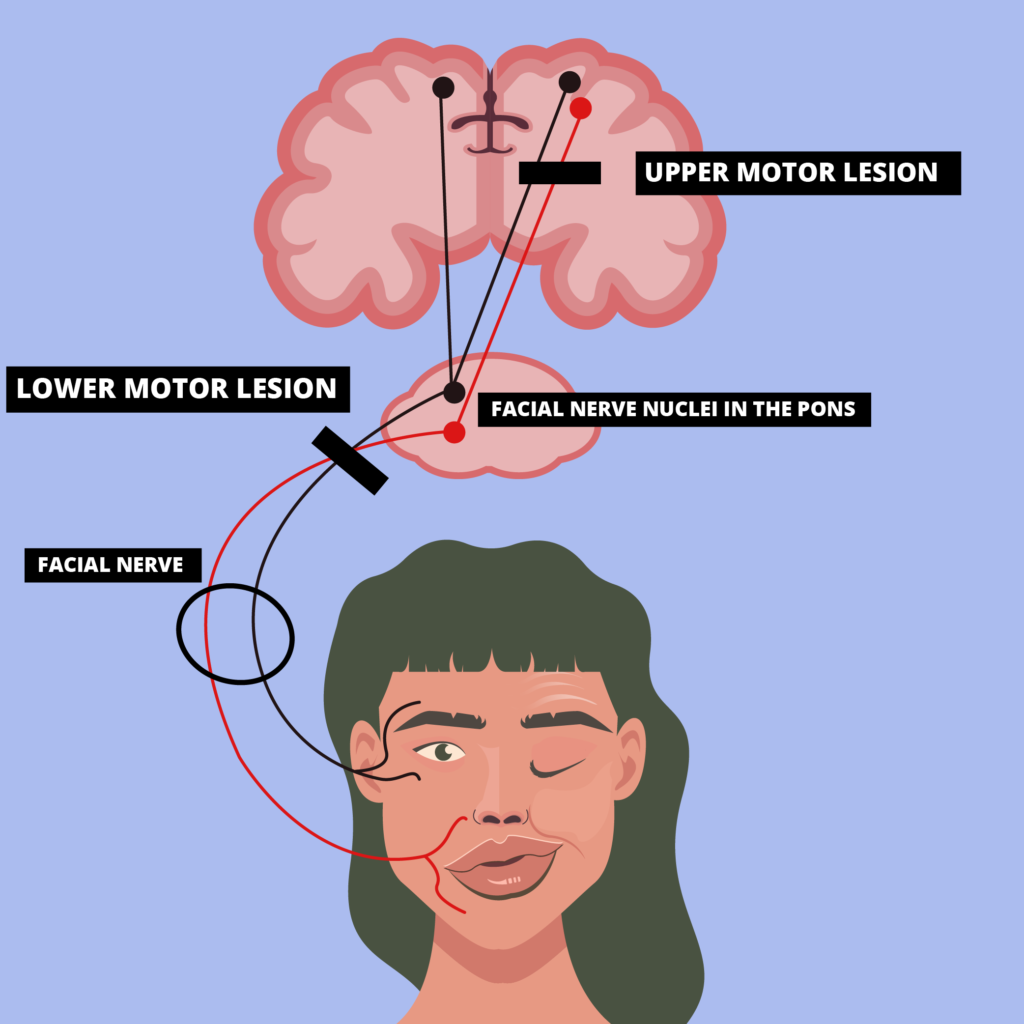
Then the lower part of the facial nuclei will lose its upper motor innervation. But the upper part of the facial nerve will be salvaged by the other half of the brain (cortex) thanks to its dual innervation.
When the cerebral cortex is damaged, in addition to the facial weakness, sometimes there could be associated arm, and leg weakness on the same side. Diseases that cause lower motor facial nerve palsies often don’t cause arm or leg paralysis except for lesions in the pons, which could produce arm and leg weakness on the opposite side.
| Feature | Upper Motor Lesions | Lower Motor Lesions |
| Facial Weakness | Only the lower half is affected | Both upper and lower halves are affected |
| Arm/Leg Weakness | On the same side | On the opposite side (In case of lesions in the pons) |
| Causes | Stroke, Tumor, Multiple Sclerosis | Pons: Tumor, StrokeCPA angle: TumorFacial canal: Ramsay Hunt syndrome, Bell’s PalsyParotid Gland: Tumor |
Causes of Upper Motor Facial Nerve palsy
- Stroke: Sudden Onset
- Tumors: Gradual Onset
- Multiple Sclerosis: Sudden onset, usually an already diagnosed patient.
Brain imaging (NCCT/MRI) can help find the exact cause.
Causes of Lower Motor Facial Nerve Palsy
Below table may seem complicated at first. But It is indeed an easy way to approach causes of Lower motor type Facial nerve palsies. The Facial nerve starts at the Pons and enters a structure called the facial canal, before branching out to supply the muscles of the face. Let’s discuss the sites of facial nerve lesions along its pathway.
| Site | Clinical Features | Causes |
| Pons | Arm, leg weakness on the opposite side of the facial palsy. (damage to the cortico-spinal tract)Cranial nerve VI palsy on the same side (Cranial nerve VI nucleus resides close to the facial nerve nucleus) | StrokeTumorMultiple Sclerosis |
| Cerbello-Pontine Angle Tumor | Associated Cranial nerve V, VI, VIIII palsiesCerebellar Signs | Tumor (Meningioma, Acoustic Neuroma) |
| Facial Canal | Isolated facial nerve palsy | |
| Parotid Gland | Lump in the Parotid Gland | Tumor |
The facial nerve originates at its nucleus in the Pons. So Pontine lesions such as Tumors, Multiple Sclerosis, and Strokes can cause Lower motor type facial nerve palsies. Since the nucleus of the Cranial Nerve VI (abducent nucleus) is situated close to that of the Facial nerve, pontine lesions are usually associated with cranial nerve VI weakness on the same side. If the adjacent cortico-spinal tracts get damaged, the patients will have arm & leg weakness on the opposite side.
CerebelloPontine Angle (CPA) is literally the space between the Pons and the Cerebellum. The facial nerve can get compressed against these two structures when there’s a CPA tumor such as Meningioma or Acoustic Neuroma. A lesion here would be characterized by associated Cranial nerves V, VI, VIII palsies and by cerebellar signs.
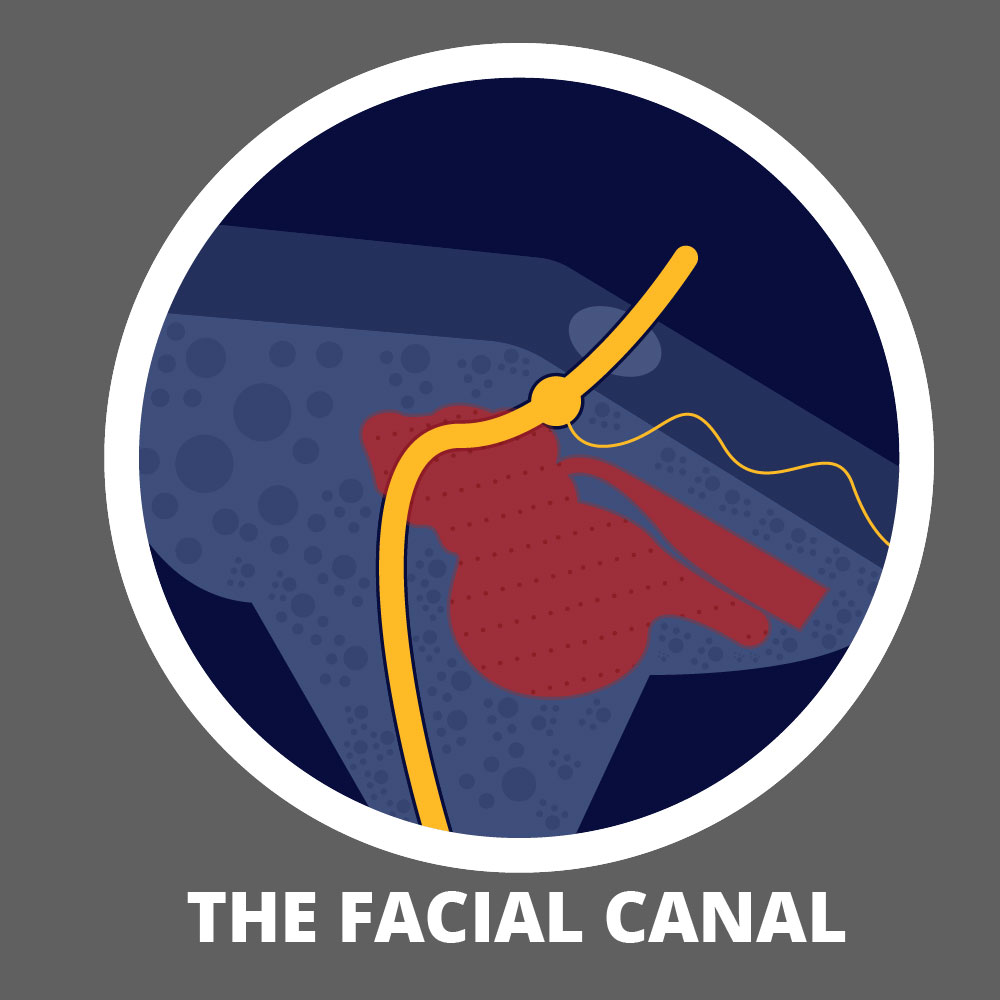
The next stop for the facial nerve is the narrow Facial canal. Since it’s very narrow, any swelling of the nerve can lead to compression of the nerve here. Here are some common causes of facial nerve palsies & associated signs.
| Cause | Associated signs |
| Bell’s Palsy | Isolated Facial nerve Palsy |
| Ramsay Hunt Syndrome | Vesicles in the ear canal |
| Lyme Disease | Tik exposure, Rash, Joint painCould be unilateral or Bilateral |
| Otitis Media | Ear discharge, Ear pain |
| Guillain Barre syndrome | Often Bilateral, |
| Sarcoidosis | Often Bilateral, Associated Pulmonary signs |
After leaving the facial canal, the facial nerve goes through the parotid gland before branching out to supply the facial muscles. Therefore palpation of the parotid glands (for tumors) is a key part of the physical examination.
Bell’s Palsy
Bell’s Palsy is the commonest cause of Facial motor weakness. It is believed to be caused by the reactivation of Herpes Simplex Virus. Inflammation of the Facial nerve at the facial canal is causing nerve compression which leads to unilateral facial muscle weakness.
- Risk Factors: Diabetes, Pregnancy, Obesity
- Clinical signs: Isolated Facial nerve palsy (lower motor type)
- Investigations: Doctors usually diagnose Bell’s palsy only with clinical findings. But there are three instances where investigations can be useful.
- Brain imaging may be useful if doctors suspect other causes like strokes or pontine lesions if the progression continues beyond three weeks, or when the recovery is delayed
- Electromyography studies may be used to assess the prognosis, in clinically complete lesions.
- Serological studies for Lyme disease are recommended in Lyme-endemic areas, especially in the presence of bilateral facial nerve palsies.
Bell’s Palsy Treatment
- In the acute stage, We start the patients on an oral steroid like Prednisolone for one week period.
- We often add antivirals like acyclovir or valacyclovir if the weakness is severe.
- If the eyes cannot be closed properly, artificial eye drops are recommended. During sleep, eyes can be carefully taped shut using medical-grade tapes. During the daytime, protective glasses can be used to minimize eye damage.
- Physical therapies like electrical stimulation of the facial muscles can be arranged to help the recovery. Though this practice is not supported by high-quality research data, many doctors including some of the cleverest neurologists I have worked under, continue to prescribe physiotherapy, especially when the recovery is prolonged.